35 yr old male with hepatic encephalopathy
A 35 yrs old male pt , resident of nakirekal, who works as a worker , brought on 14/12/21 with the chief complaints of


 pitting edema
pitting edema

 subcongetival hemorrhage
subcongetival hemorrhage



 SAAG , serum electrolytes , serum creatinine
SAAG , serum electrolytes , serum creatinine







Unresponsiveness since morning he brought
Swelling of legs ( pedal edema) since 4 days
Abdominal distension since 5 days
Yellowish discoloration of scleral and eyes since 6 months
History of present illness :
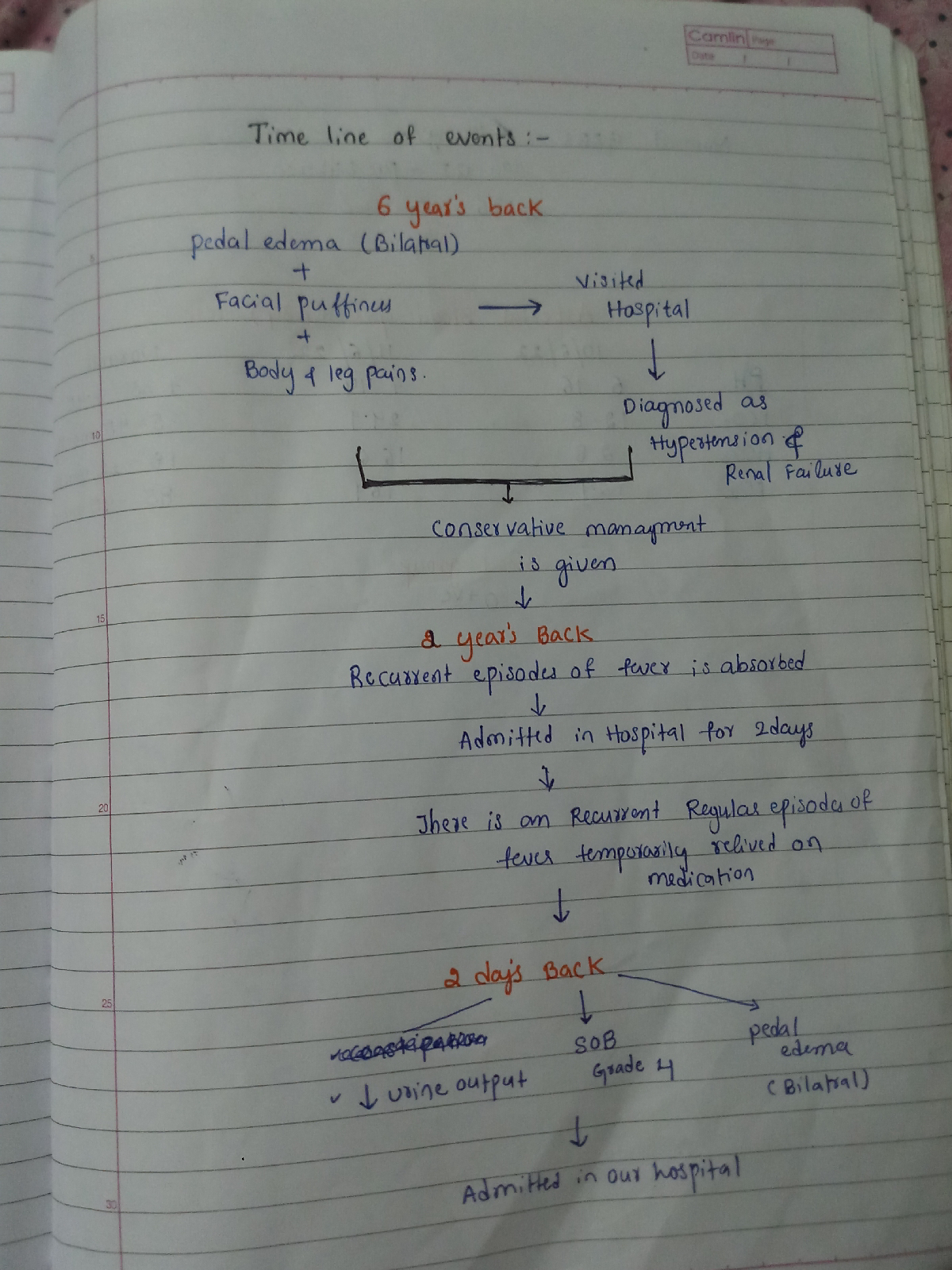
1. Pt was apparently asymptomatic 6 years back .. then he developed fever for 2 days, followed by altered behaviour with jaundice
Pedal edema and abdominal distension
2 . They went to the hospital admitted for 5 days , where the diagnosed it as chronic liver disease (CLD )
3 . He is a chronic alcohol for 20 years
4 . Treatment was given... and he is good for 2 years
5 . Then in 2017 ( after 2 yr )
He developed similar symptoms.. but there is no fever
6 . Then he visited to other hospital and used medications regularly for 6 months...
7 . Then he was irregular on medication and continued taking alcohol intermittently
8 . Then few days back.. he had loose stools ( 4 to 5 episodes per day )
9 . Then he developed fever since 5 days ..
As now there is no fever as it is subsided by 4 tablets of dolo
10 . Then 3 days back.. presented with the hospital with the chief complaints of
Altered sensorium: not responding to the commands
Abdominal distension
Pedal edema
. Chief complaints of nausea and loss of appetite
Yellow discoloration
Negative history :
No history of weakness , involuntary moments
No history of Malena, pain abdomen
Past history :
Not a known case of DM ,HTN, Asthma, coronary artery disease
He is a known case of pulmonary koche 15 years back used ATT
Personal history :
Mixed diet
Chronic alcoholic since 20 years
No smoking, no known Allergies
Family history :
No similar complaints
Father has asthma..from 15 years... he died due to paralysis few days back ...
Mother was know case of diabetes
General examination :
Pt is conscious,coherent and cooperative.thin built and malnourished.
No pallor
icterus is present
No clubbing
No lymphadenopathy
Pedal edema is present

Vitals :
Temp : Afebrile
BP : 100/80 mm Hg
PR : 105 bpm
RR : 25 cpm
GRBS : 33 mg / dl
SpO2 : 91 % @ RA
Systemic Examination :
CVS : S1S2 + , No murmurs
RS : BAE + , NVBS +
P/A : Soft , Nontender , BS +
CNS : Response to pain
Provisional diagnosis :
HEPATIC ENCEPHALOPATHY grade 4 SECONDARY TO LIVER FAILURE
Spontaneous Bacterial Peritonitis
Grade 2 Espophageal Varices
Derranged Coagulation Profile
?Prerenal AKI (?Hepatorenal Syndrome)
Hypokalemia
RECURRENT HYPOGLYCEMIA
K/C/O CHRONIC LIVER DISEASE WITH GROSS ASCITES AND SPLENOMEGALY(PORTAL HTN)
Investigation :
Fever chart




0n 14/ 12 /21
Liver function test

Blood sugar is 71 mg/dl ( 100 to 160 )
and blood urea is 58 mg / dl ( 12 to 42 )
On 16 / 12 / 21
Ecg :
Plan of Treatment :
INJ.LASIX 20 MG/IV/BD
TAB.ALDACTONE 50 MG/RT/BD
INJ.25% DEXTROSE 100ML/IV/SOS IF GRBS<60 MG/DL
SYP. LACTULOSE 20 ML/PO/BD
INJ. THIAMINE 1 AMP IN 100 ML NS/IV/TID
GRBS CHECK HOURLY
BP/PR/TEMP CHARTING HOURLY
T. UDILIV 300 MG/ RT/BD
SYP. HEPAMERZ 2 TBSP/RT/BD
T RIFAXIMIN 550 MG /RT/BD
ENEMA 12 TH HOURLY
STRICT I/O CHARTING
INJ.CEFOTAXIME 2G /IV/BD

{kind=link}
{kind=link}