28 years old Male with uremia encephalopathy with ckd on maintenance hemodialysis (MHD)
A 28 year old male pt , resident of nalgonda district who is a sales man in cloth store, presented to casualty ( on 22/12/21) with the chief complaints of
A. Seizures
H/o seizures 3 episodes around 3am, 7am, 11am. Each episode lasting for 3-5 min associated with uprolling of eyeballs, frothing from mouth.
Not associated toungue bite, involuntary micturition, involuntary defecation, lethal cry.
Followed by post ictal confusion lasting for 15-20 mins
B . H/o fever 1 week back associated with chills .
C . H/o sob since 10 days, grade II - III.
D . H/0 chest pain since 3 days
D . Negative history
No H/o hematuria , frothy urine, nausea, loose stools, decreased urine output, pedal edema.
( but there is history of vomiting during dialysis on 23rd)
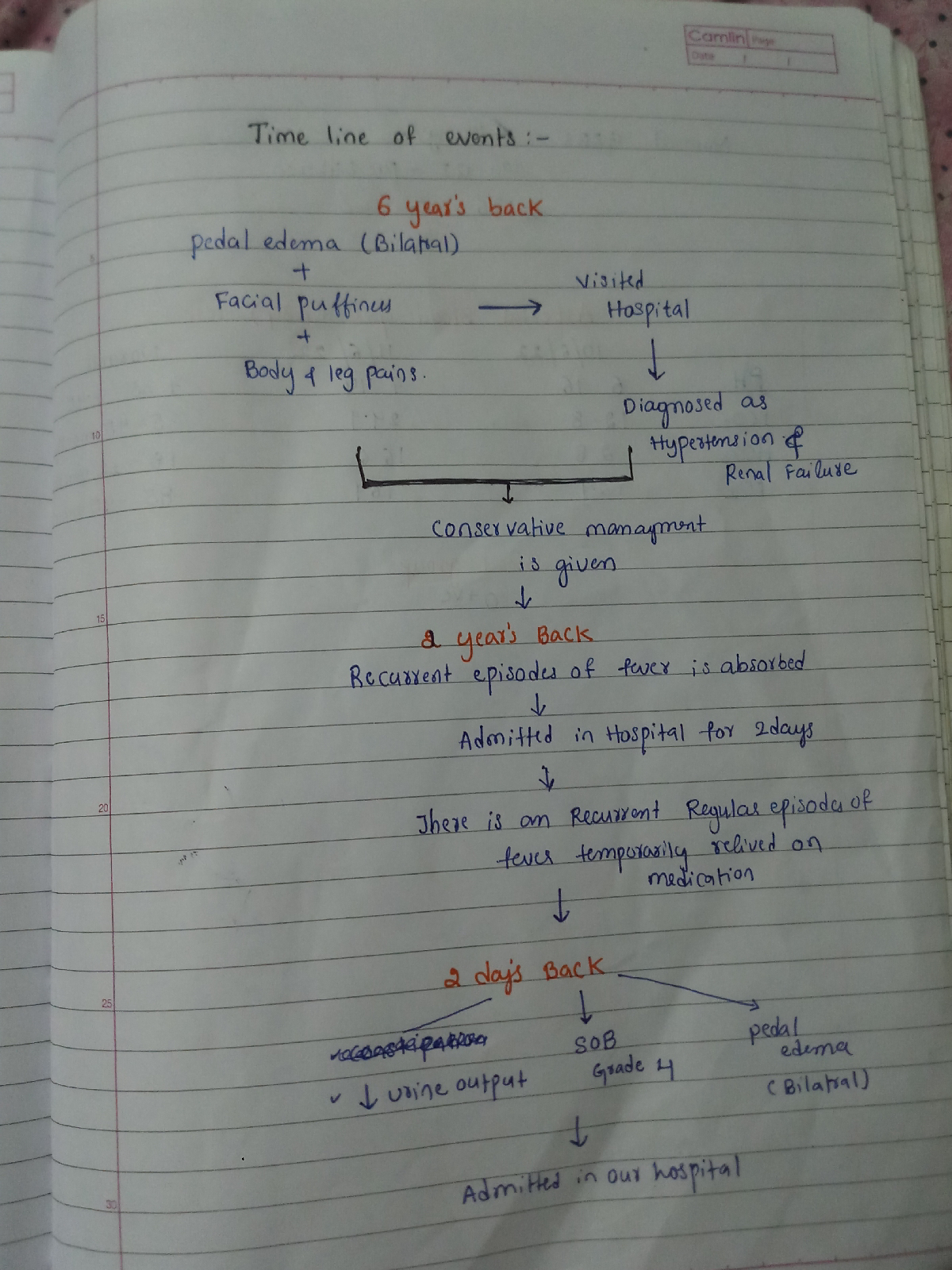
History of present illness:
Pt was apparently asymptomatic 10 (February 2021)months back then
1) he noticed sudden loss of weight of about 10-15kgs, in a span of 1 & 1/2 months 2) for which he consulted local doctor where he was diagnosed to have CKD and his creatinine levels are high
3) for which he was advised to undergo dialysis I /v/o high creatinine levels.
4) he went to other hospital in Hyderabad and they tested and told him he was HYPERTENSIVE along with decreased kidney size and suggested dialysis
5 ) he came to our hospital for dialysis , here he tested COVID + in APRIL 2021 , then he came back for dialysis after 2 months on JUNE 24TH
6 ) K/c/o CKD since April 2021 and is on MHD since June underwent 27 sessions of hemodialysis., Discontinued from 19/10/21 ( SEPTEMBER)
7 ) then he presented with fever, seizures on DECEMBER, where the dialysis was done 5 sessions till 10 / 1 / 22
He had a altered behaviour....and confusing about place and trying to take the cannula on the 3 to 4 days of admitting ( 22/ 12 / 21 )
Past history :
K/c/o HTN +.since 8 months.
Not a k/c/o DM, CAD, ASTHMA, TB.
Personal history:
Diet: mixed .
Appetite: reduced
B&b: regular.
Sleep: adequate.
No significant family history.
On examination:
Pt is c/c/c moderately built with mild dehydration.
A ) Pallor +, B) no signs of icterus, cyanosis, clubbing, lymphadenopathy, pedal edema.
C ) Temp: 98.6 f
PR: 88 bpm
RR: 14 cpm
BP: 160/100 mm hg
SpO2: 98% @ RA
GRBS : 130 mg%
CVS: S1, S2+ no murmurs
RS: BAE+, NVBS+
Pleural rub is present
P/A: SOFT, NON TENDER.
CNS: PT IS CONSCIOUS
SPEECH: NORMAL
NO SIGNS OF MENINGEAL IRRITATION.
REFLEXES: R. L.
B. 2+. 3+
T. 3+. 3+.
S. -. 3+.
K. 3+. 3+
A. -. -.
P. REDUCED
POWER: R. L.
UL. 5/5. 5/5
LL. 5/5. 5/5
TONE:. R. L.
UL. N. N.
LL. N. N.
Gait: normal
Provisional diagnosis : UREMIC ENCEPHALOPATHY WITH CKD ON MHD
CKD ON MHD WITH DIALYSIS DYSEQUILIBRIUM SYNDROME, WITH HYPERTENSIVE NEPHROPATHY WITH K/C/O HTN.
Clinical pictures: